Clinical caution
PE decision rules support clinical judgment; they do not replace it. Do not delay urgent imaging, anticoagulation decisions, or advanced therapy consideration in patients with shock, syncope, severe hypoxemia, right-heart strain, or high clinical suspicion for massive pulmonary embolism.
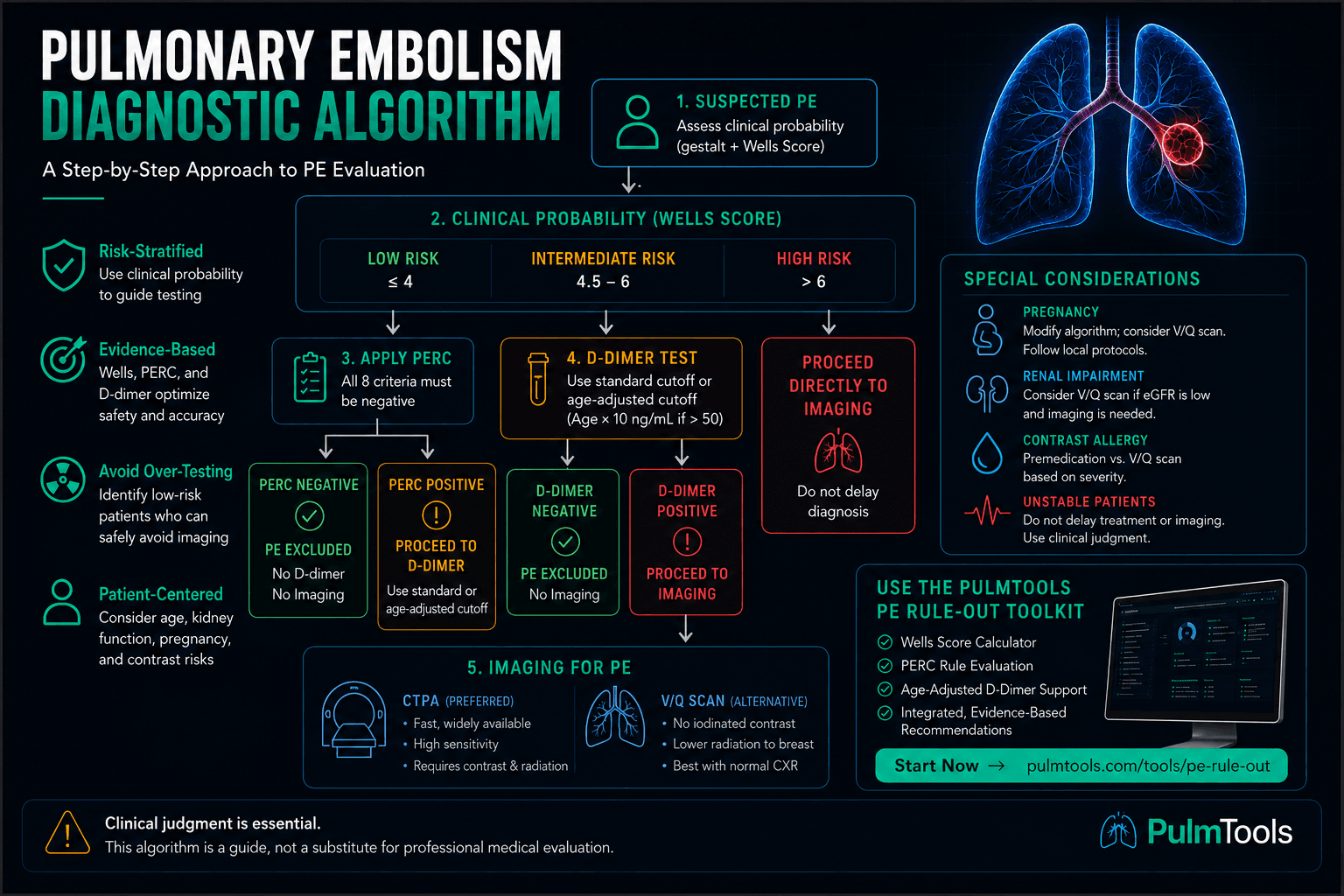
Pulmonary embolism diagnosis is not a single test decision. It is a sequence: recognize concerning PE symptoms and clinical clues, estimate pretest probability, decide whether the patient is low enough risk for PERC, use D-dimer only when it can safely reduce imaging, then choose the right imaging strategy when PE cannot be excluded.
Pulmonary embolism diagnostic algorithm
The safest PE rule-out pathway begins before the lab order. A D-dimer is powerful in the right patient and noisy in the wrong one. The key is matching the test to the patient's clinical probability and recognizing common D-dimer false positives before overreacting to an isolated positive result.
Step 1: assess clinical probability before testing
Start with the patient in front of you: symptoms, vital signs, risk factors, clinical clues, competing diagnoses, exam findings, and whether PE is the most likely explanation. The Wells Score for pulmonary embolism gives structure to that judgment and helps separate low, intermediate, and high probability pathways.
Practical interpretation
- Low probability: consider PERC first if the clinician's suspicion is low enough. For the bedside sequence, see the low-risk PE rule-out pathway.
- Intermediate probability: D-dimer can be useful; PERC should not be the main exclusion step.
- High probability: do not rely on D-dimer to rule out PE. If the patient is PE likely by two-tier Wells, proceed toward definitive imaging or urgent management.
Step 2: low-risk patients can be screened with PERC
The PERC rule is designed for patients who are already low risk. If all eight PERC criteria are negative, PE can often be ruled out without D-dimer or imaging. That is the point: avoid unnecessary downstream testing in a patient whose baseline probability is already very low.
PERC should not be forced onto patients with moderate or high suspicion. If the patient looks clinically concerning, has abnormal physiology, or PE is a serious competing diagnosis, move beyond PERC.
Step 3: use D-dimer when it can safely change the plan
D-dimer is sensitive but nonspecific. A negative result can help exclude PE in appropriate low- or intermediate-risk patients. A positive result does not diagnose PE; it means the pathway usually continues to imaging or additional evaluation.
D-dimer becomes much less useful when the pretest probability is high because a negative result may not safely lower risk enough to stop the workup. It also becomes less specific in older adults, pregnancy, cancer, infection, trauma, surgery, hospitalization, and inflammatory states. See D-dimer false positives for a dedicated breakdown of elevated D-dimer without PE.
Step 4: apply age-adjusted D-dimer when appropriate
In patients older than 50, an age-adjusted D-dimer threshold can reduce false positives and unnecessary imaging. A common FEU-based approach is:
Age-adjusted D-dimer formula
Age × 10 ng/mL FEU
Examples: age 60 → 600, age 75 → 750, age 82 → 820 ng/mL FEU.
Some pathways use alternatives such as the YEARS algorithm, which adjusts D-dimer interpretation based on specific clinical criteria rather than age alone.
Step 5: image when PE cannot be excluded
If clinical probability and D-dimer testing do not exclude PE, the next step is usually imaging. The imaging question often becomes CTPA vs V/Q scan. CT pulmonary angiography is commonly used because it is fast, widely available, and provides direct anatomic evaluation of pulmonary arteries.
V/Q scanning remains important when iodinated contrast is a problem, renal function is a concern, pregnancy-specific protocols favor it, or local imaging pathways recommend it. A normal or near-normal chest X-ray generally improves the usefulness of V/Q interpretation, while abnormal lung parenchyma can make V/Q results harder to act on.
Special circumstances: pregnancy, renal dysfunction, and contrast allergy
Pregnancy, renal impairment, and contrast allergy can change the imaging decision. These patients often need protocol-specific pathways rather than a generic rule-out flowchart. Local radiology, emergency medicine, obstetric, and pulmonary/critical care protocols matter here.
The same diagnostic principles still apply: estimate pretest probability, avoid unnecessary tests when safe, and do not let a rule delay care when PE is clinically dangerous.
Unstable patients are not rule-out-tool patients
A patient with hypotension, shock, severe hypoxemia, syncope with concern for PE, escalating oxygen requirement, or evidence of right heart strain requires urgent evaluation. Decision tools should not slow the team down. In these situations, bedside echocardiography, emergent imaging when feasible, anticoagulation decisions, and PE response team activation may matter more than outpatient-style diagnostic branching.
PulmTools clinical workflow
Use the PE Rule-Out Toolkit
Run Wells Score, PERC, D-dimer logic, and age-adjusted D-dimer in a single clean workflow. The toolkit keeps PERC de-emphasized when Wells risk is no longer low, helping match the interface to actual bedside reasoning. For a focused bedside workflow, review the low-risk PE rule-out pathway.
Related PE resources
PE Rule-Out Toolkit
Run Wells Score, PERC, and D-dimer logic in one bedside-friendly PE rule-out workflow.
Read moreWells Score for Pulmonary Embolism
Understand PE pretest probability before ordering D-dimer or imaging.
Read morePERC Rule for Pulmonary Embolism
Learn when low-risk patients can avoid D-dimer and imaging entirely.
Read moreAge-Adjusted D-Dimer
Calculate age-adjusted D-dimer thresholds and reduce unnecessary imaging in older adults.
Read moreD-Dimer for Pulmonary Embolism
Understand when D-dimer helps rule out PE and why positive results are nonspecific.
Read moreD-Dimer False Positives
Review infection, inflammation, age, cancer, pregnancy, trauma, and other causes of elevated D-dimer.
Read moreYEARS Algorithm for Pulmonary Embolism
Compare Wells-based pathways with YEARS-style D-dimer threshold strategies.
Read moreCTPA vs V/Q Scan
Compare imaging choices when PE cannot be excluded by clinical pathway or D-dimer.
Read morePE Symptoms and Clinical Clues
Review the symptoms, signs, and risk factors that should trigger formal PE evaluation.
Read moreFrequently asked questions
What is the first step in evaluating suspected pulmonary embolism?
The first step is assessing clinical probability using clinician gestalt and/or a validated tool such as the Wells Score. The pretest probability determines whether PERC, D-dimer testing, or imaging is appropriate.
When should the PERC rule be used?
The PERC rule should only be used in patients who are already considered low risk for pulmonary embolism. It should not be applied to moderate-risk, high-risk, unstable, or clinically concerning patients.
When should a D-dimer be ordered for pulmonary embolism?
D-dimer is most useful in low-risk or intermediate-risk patients when pulmonary embolism is possible but not highly likely. A negative D-dimer can help exclude PE in appropriate patients, but a positive result usually requires further evaluation.
What is an age-adjusted D-dimer?
Age-adjusted D-dimer uses a higher cutoff in patients older than 50 years, commonly age multiplied by 10 ng/mL FEU. For example, a 70-year-old patient may have an age-adjusted cutoff of 700 ng/mL FEU.
When is CTPA preferred over a V/Q scan?
CT pulmonary angiography is often preferred when rapid anatomic imaging is needed and the patient can receive iodinated contrast. V/Q scanning may be considered when contrast allergy, renal dysfunction, pregnancy considerations, or local protocols make CTPA less desirable.
Should PE decision rules be used in unstable patients?
Decision rules should not delay urgent evaluation, imaging, anticoagulation decisions, or advanced therapy consideration in patients with hemodynamic instability or high suspicion for massive pulmonary embolism.
This educational resource is for clinical learning and workflow support only. Always follow local protocols, supervising clinician direction, and patient-specific risk assessment.