Ventilation Physiology
Alveolar Ventilation, Dead Space, and CO₂ Clearance Explained
Learn how alveolar ventilation, anatomic dead space, and the VD/VT ratio affect carbon dioxide clearance. This guide connects the formulas to bedside respiratory care, ABG interpretation, and ventilator decision-making.
Tool
Minute & Alveolar Ventilation
Calculate V̇E and V̇A using tidal volume, respiratory rate, and dead space.
Tool
Dead Space Calculator (VD/VT)
Estimate VD/VT ratio and dead space volume using PaCO₂, ETCO₂, and tidal volume.
Tool
ABG Analyzer
Interpret PaCO₂ and acid-base changes in the full clinical context.
Why alveolar ventilation matters
Minute ventilation tells you the total amount of air moving in and out of the lungs each minute. It is calculated as tidal volume multiplied by respiratory rate. That number is useful, but it does not tell you how much air is actually reaching functioning alveoli.
Alveolar ventilation is more clinically important for carbon dioxide clearance because it subtracts the part of each breath that is lost to dead space. In plain terms, a patient can have a seemingly acceptable minute ventilation and still retain CO₂ if too much of that ventilation is wasted.
This is why clinicians often move beyond simple respiratory rate and tidal volume math and look at the relationship between dead space, alveolar ventilation, and the patient’s PaCO₂ on the ABG.
Core formulas to know
Minute Ventilation (V̇E)
VT × RR
Total air moved per minute. Helpful, but incomplete when assessing effective gas exchange.
Alveolar Ventilation (V̇A)
(VT − VD) × RR
The portion of ventilation that actually reaches alveoli and participates in gas exchange.
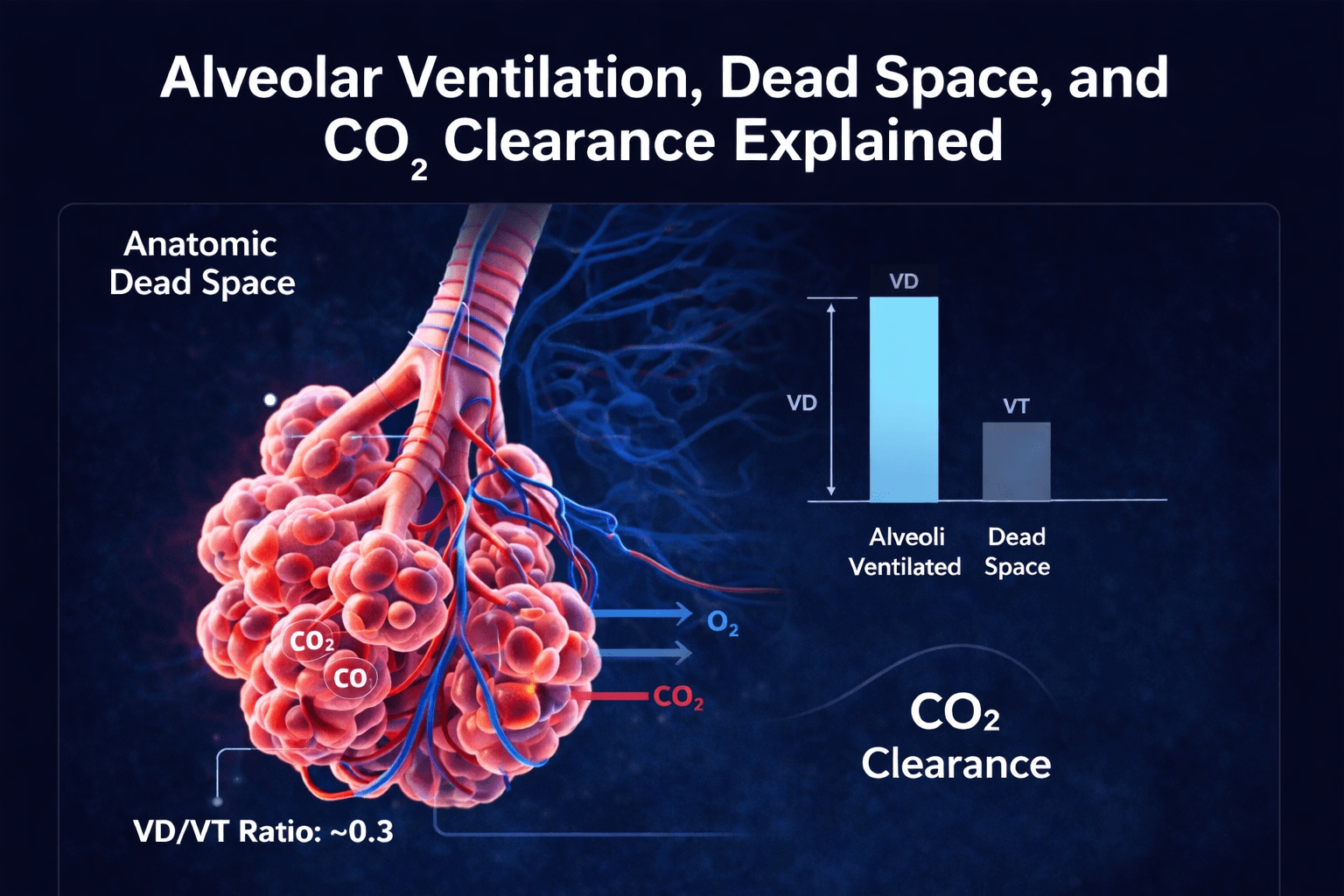
Dead Space Fraction (VD/VT)
(PaCO₂ − ETCO₂) / PaCO₂
A bedside estimate of how much of each breath is wasted ventilation. This helps explain ventilation inefficiency and why CO₂ clearance may be worse than expected.
What is anatomic dead space?
Anatomic dead space is the portion of inspired air that remains in the conducting airways and never reaches alveoli. This includes the nose, mouth, trachea, bronchi, and other airways that conduct gas but do not perform gas exchange.
In many adult bedside calculations, anatomic dead space is estimated at roughly 150 mL. That shortcut is useful for fast mental math, but it is still an estimate. Body size, airway anatomy, artificial airways, and disease state all affect the true number.
There is also physiologic dead space, which includes anatomic dead space plus alveoli that are ventilated but not effectively perfused. In critically ill patients, physiologic dead space can increase substantially and may become far more clinically important than the simple 150 mL estimate.
How to estimate dead space at the bedside
For quick respiratory care calculations, many clinicians begin with an anatomic dead space estimate of about 150 mL in an adult. That works reasonably well for teaching, quick checks, and simple alveolar ventilation math.
When you need a more clinically useful estimate of wasted ventilation, the dead space calculator lets you use PaCO₂ and ETCO₂ to estimate a VD/VT ratio. This moves you from a generic assumption toward a more patient-specific look at ventilation efficiency.
That distinction matters. A patient with high physiologic dead space may need more total ventilation to achieve the same PaCO₂ target, which is one reason your desired VE calculation can look fine on paper but still feel mismatched at the bedside.
Clinical pearl
When dead space rises, the patient may require more total minute ventilation just to maintain the same alveolar ventilation and PaCO₂. That is why two patients with identical tidal volume and respiratory rate can have very different blood gas results.