Clinical Management
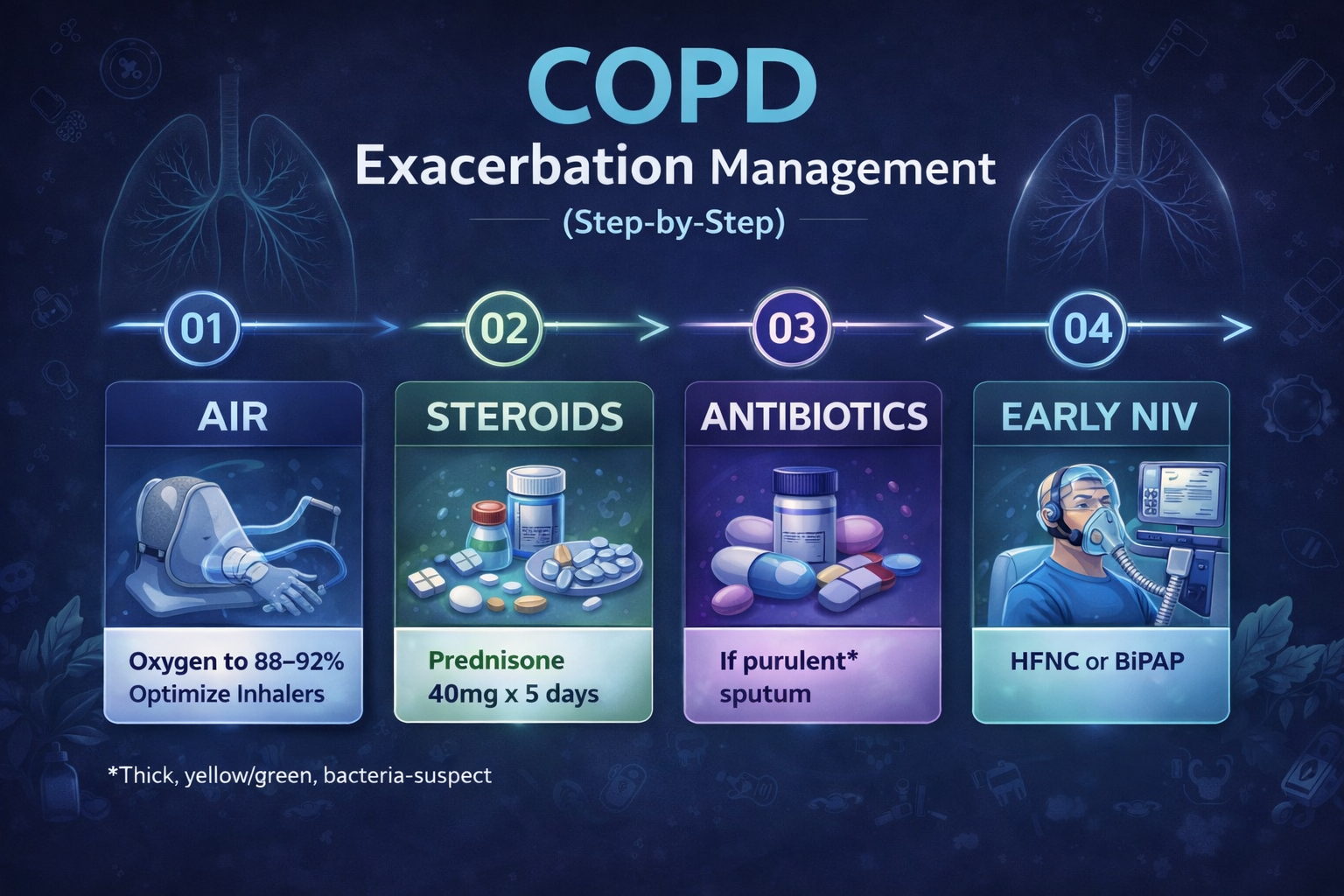
COPD Exacerbation Management (Step-by-Step)
A practical, step-by-step guide to COPD exacerbation management, including oxygen targets, bronchodilators, steroids, antibiotics, noninvasive ventilation, and when to escalate care.
Quick Summary
- Target oxygen saturation carefully, often around 88–92% when CO₂ retention is a concern.
- Start short-acting bronchodilators early and reassess work of breathing frequently.
- Systemic steroids shorten recovery and reduce treatment failure in many exacerbations.
- Antibiotics are most useful when sputum is purulent, volume increases, or ventilatory support is needed.
- Use early NIV/BiPAP for acute hypercapnic respiratory failure when indicated.
What is a COPD exacerbation?
A COPD exacerbation is a sustained worsening in respiratory symptoms beyond day-to-day baseline, often involving increased dyspnea, cough, sputum production, or sputum purulence. These episodes can be triggered by infection, environmental exposures, poor medication adherence, or other cardiopulmonary problems.
A good COPD exacerbation workflow balances symptom control, oxygenation, ventilation, and rapid identification of patients who need escalation.
Step 1: Oxygen and Initial Assessment
- Assess mental status, respiratory rate, work of breathing, and accessory muscle use.
- Check pulse oximetry and consider ABG or VBG when ventilation or acid-base status is unclear.
- Titrate oxygen thoughtfully. In many COPD exacerbations, a target of 88–92% is used when hypercapnia is a concern.
- Look for alternative or overlapping diagnoses: pneumonia, pneumothorax, CHF, PE, or ACS.
If you need help interpreting worsening gases, pair this page with our ABG Interpretation Guide and Mastering ABG Analysis.
Step 2: Bronchodilators
- Use short-acting beta agonists early.
- Short-acting anticholinergics are also commonly added.
- Metered-dose inhaler with spacer may work well in milder cases; nebulizers are often used when distress is higher.
- Reassess response after treatment rather than assuming one round is enough.
Step 3: Steroids
Systemic steroids are a core part of COPD exacerbation management in many patients. A common regimen is:
Steroids can shorten recovery, improve lung function, and reduce treatment failure.
Step 4: Antibiotics
Antibiotics are not needed for every COPD exacerbation, but they are often used when:
- Sputum becomes more purulent
- Sputum volume increases
- Dyspnea significantly worsens
- Mechanical ventilation or NIV is required
If sputum is thick, yellow, or green and the overall picture suggests bacterial infection, antibiotics become more reasonable.
Step 5: NIV, HFNC, and Escalation
- Use early NIV/BiPAP when acute hypercapnic respiratory failure is present.
- Watch pH, PaCO₂, mental status, fatigue, and work of breathing closely.
- HFNC may help some patients, but NIV remains a key therapy in hypercapnic COPD exacerbation.
- Escalate to intubation when NIV fails, the airway is not protected, or deterioration continues.
For a deeper comparison of interfaces and escalation decisions, see our HFNC vs BiPAP/NIV guide.
Disposition and Follow-Up
- Discharge may be appropriate if oxygenation is stable, distress has improved, and home support is adequate.
- Admission is more likely with persistent hypoxemia, acidosis, fatigue, altered mental status, or repeated bronchodilator need.
- Before discharge, confirm inhaler access, technique, steroid plan, and return precautions.
Related PulmTools COPD Cluster
FAQ
What oxygen saturation should I target in a COPD exacerbation?
When hypercapnia is a concern, many clinicians use a target of 88–92% rather than chasing higher saturations.
When should antibiotics be used?
Antibiotics are most helpful when sputum becomes purulent, sputum volume rises, dyspnea worsens, or ventilatory support is needed.
Is NIV better than HFNC in a hypercapnic COPD exacerbation?
NIV/BiPAP remains a key first-line therapy in acute hypercapnic respiratory failure from COPD exacerbation.
References & Further Reading
- Official GOLD reports and executive summaries
- Hospital COPD exacerbation pathways and respiratory care protocols
- ABG, oxygenation, and NIV guidance relevant to hypercapnic respiratory failure