Advanced Oxygenation & ARDS
Inhaled Nitric Oxide: What Actually Works (and What Doesn’t)
Inhaled nitric oxide (iNO) is widely used in critical care, but often misunderstood. This guide breaks down the one evidence-based indication, the common off-label uses, and how iNO actually affects V/Q matching in ARDS.
Tool
P/F Ratio & OI
Assess oxygenation severity in ARDS.
Tool
ROX Index
Evaluate HFNC response and failure risk.
Tool
ABG Analyzer
Interpret oxygenation and CO₂ together.
What is inhaled nitric oxide?
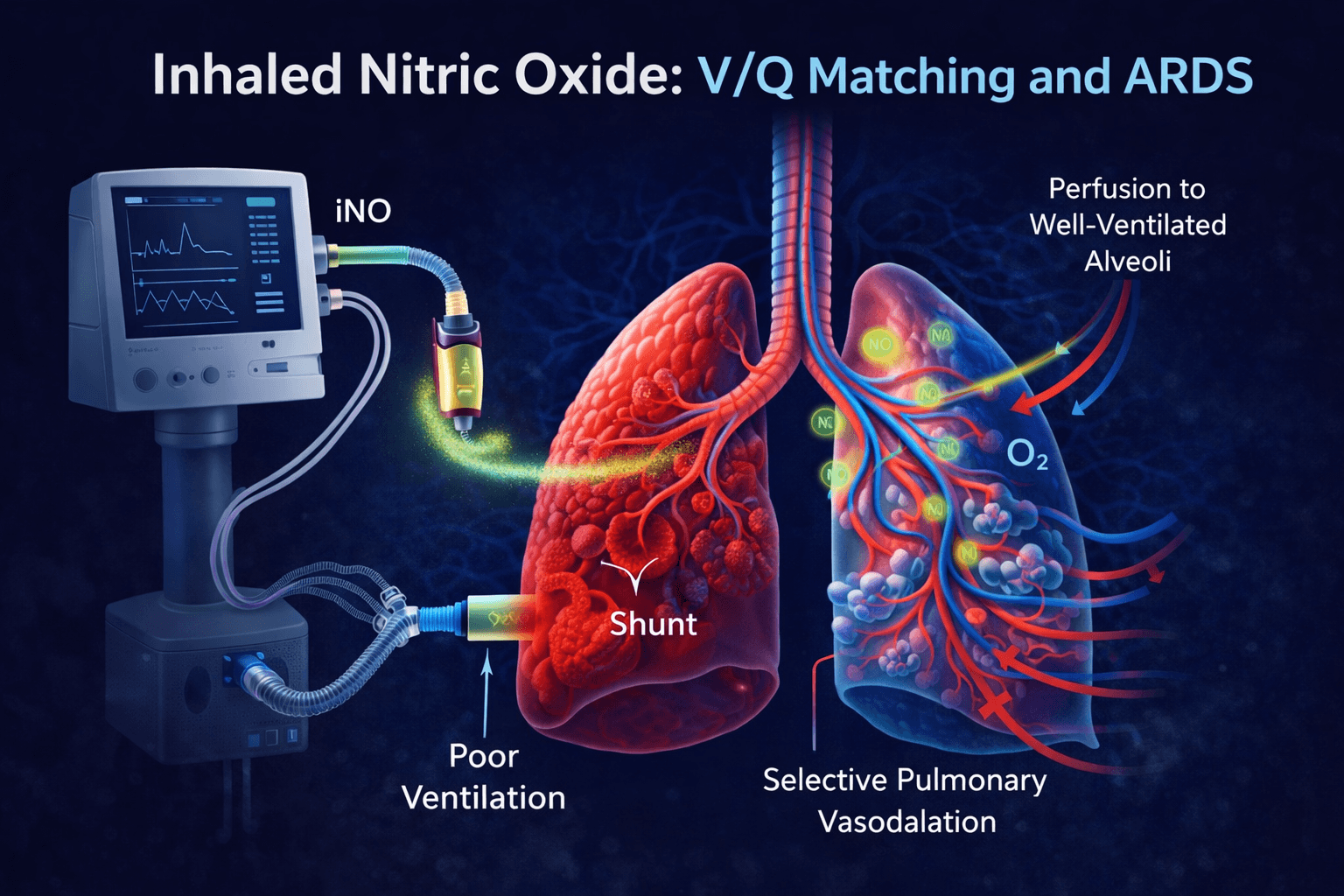
Inhaled nitric oxide (iNO) is a selective pulmonary vasodilator that improves oxygenation by redirecting blood flow toward well-ventilated alveoli. It enhances ventilation-perfusion (V/Q) matching without causing systemic hypotension.
How it works
Nitric oxide is delivered via the ventilator circuit and diffuses into pulmonary vasculature. It selectively dilates vessels in ventilated regions, improving oxygen uptake and reducing shunt.
- • Improves V/Q matching
- • Reduces intrapulmonary shunt
- • Enhances oxygenation transiently
The only true evidence-based use
The strongest evidence for inhaled nitric oxide exists in neonatal hypoxic respiratory failure, where it reduces the need for ECMO. In adults, the story is different.
Use in ARDS
In ARDS, inhaled nitric oxide can improve oxygenation temporarily, but studies consistently show no mortality benefit. It should be viewed as a bridge therapy, not a solution.
Common off-label uses
- • ARDS rescue therapy
- • Right ventricular failure
- • Pulmonary hypertension
- • Bridge to ECMO
Limitations and risks
- • No proven mortality benefit in adults
- • Expensive
- • Risk of rebound hypoxemia
- • Methemoglobinemia (rare)
Clinical takeaway
Inhaled nitric oxide improves oxygenation — but improving oxygenation is not the same as improving outcomes. Use it thoughtfully, reassess frequently, and always pair it with a full clinical picture.